COVID-19
Vaccination
John Jacobs, 6th March 2021.
Looking back at historical developments like the AIDS vaccine development, I predicted it would take many years before we would have had a vaccine. However, science and the pharmaceutical industry have shown that new technologies can work surprisingly well. This gives hope for the many other infectious diseases where we still do not have vaccines.
Vaccine production is slow.
Nobody wants the disease caused by the SARS-2 virus. So virtual all with medical knowledge prefer to be vaccinated against COVID-19. Normally it could take a long time for a vaccine to be produced after approval, but pending possible approval, the EU encouraged pharmaceutical companies to start production already. The first three vaccines have now been approved in the EU, and a fourth is approved in the USA and submitted in the EU. The mRNA vaccines from Moderna and Pfizer protect more than expected about 95% in the trials and AstraZeneca 60%. Johnson & Johnson (Janssen) might be 66% according to the FDA. Europe has distributed the vaccines fairly among the various countries, but it is likely that it takes all of 2021 to have everyone protected by vaccination (Figure 1).
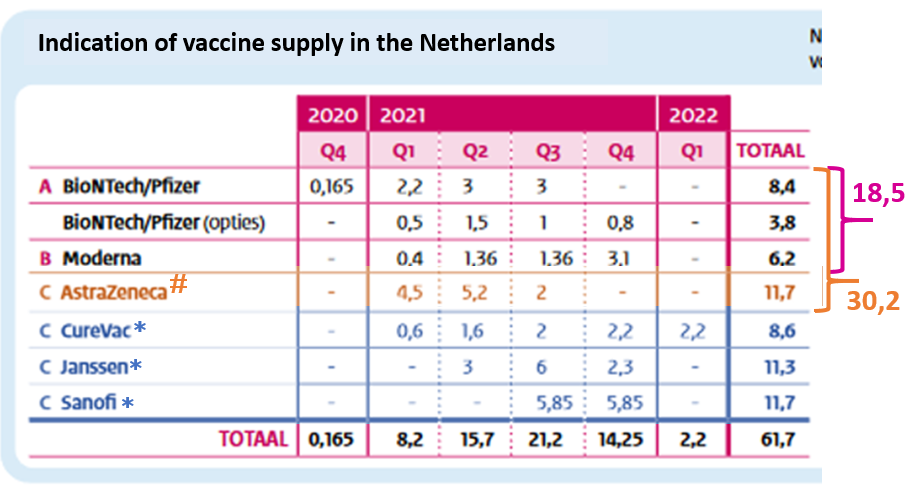
Figure 1. Indication of COVID-19 vaccines supply in the Netherlands.
The Netherlands has a population of 17 million that must be vaccinated twice for optimal protection. # Not tested on persons> 55 years old. * No test results yet. The totals promised in 2021 are shown on the right. Similar data relative to their population are implied for other EU countries.
The Netherlands has a population of 17 million that must be vaccinated twice for optimal protection. # Not tested on persons> 55 years old. * No test results yet. The totals promised in 2021 are shown on the right. Similar data relative to their population are implied for other EU countries.
The Dutch vaccination plan.
Earlier I wrote about the Dutch virus and that seems to be reflected in the vaccination plan in the Netherlands (Figure 2). The prioritization of care workers over vulnerable people is striking. Even a major part of the normal population will be vaccinated before many of the vulnerable people. It appears that European ethical considerations are irrelevant for the Netherlands.
Against the European principles of vaccinating the weaker and vulnerable first, the Netherlands started vaccinating employees in nursing homes, care for the disabled, home care and COVID-19 care, before vaccinating the first residents. Marion Koopmans warned against unnecessary vaccinations of care workers (Figure 4). In the polder model, politicians seem to be more sensitive to lobbyists than to facts from the EMA, MEB and the Dutch Health Council, which ultimately issued its advice four times.
Against the European principles of vaccinating the weaker and vulnerable first, the Netherlands started vaccinating employees in nursing homes, care for the disabled, home care and COVID-19 care, before vaccinating the first residents. Marion Koopmans warned against unnecessary vaccinations of care workers (Figure 4). In the polder model, politicians seem to be more sensitive to lobbyists than to facts from the EMA, MEB and the Dutch Health Council, which ultimately issued its advice four times.
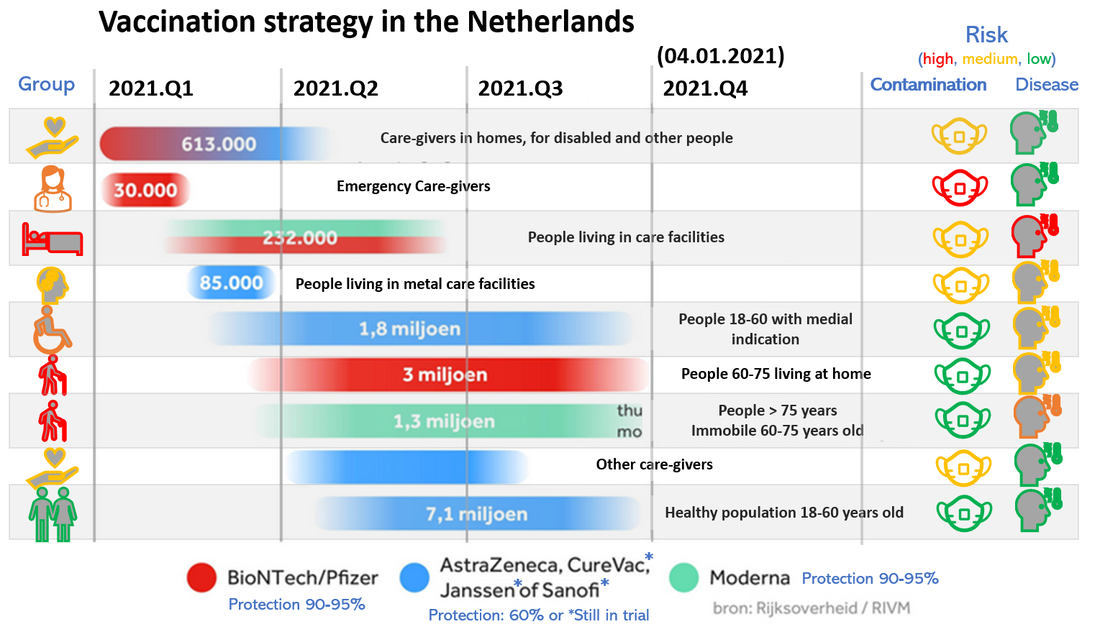
Figure 2. Vaccination strategy in the Netherlands. Information is from the national government.
Later, priority is shifted even more to care workers. I have included the risk assessment for contamination and infection for comparison of the groups. The schedule indicates the start of vaccination, protection is achieved 6 weeks after vaccination.
Later, priority is shifted even more to care workers. I have included the risk assessment for contamination and infection for comparison of the groups. The schedule indicates the start of vaccination, protection is achieved 6 weeks after vaccination.

Figure 3. Warning by Prof. Koopmans when people with vital functions would be vaccinated prior to vulnerable people.
Vaccination of people is also mentioned in the opinion because of instant maintenance of vital functions. That choice is also important, but also a difficult one. Where do you draw the line? 1.4 million people (8%) work in care and welfare.
Vaccination of people is also mentioned in the opinion because of instant maintenance of vital functions. That choice is also important, but also a difficult one. Where do you draw the line? 1.4 million people (8%) work in care and welfare.
Ethics of competing interests
Vaccination is important for everyone because it protects health. Vulnerable people, such as the elderly, have a greater interest in vaccination in QALYs than less vulnerable people, because of a hight risk of fatal outcome. The tables are turned in case of ICU admission. IF one starts from the equality of people vulnerable people should be given priority in vaccination, as agreed in the EU and is also carried out in many other Western countries, such as the United Kingdom and Israel.
Previously, there has been international criticism on the exclusion of older and frail people from vaccination and treatment studies for COVID-19. These people should be the target of the vaccination, and so vaccination should be tested to see if it is effective for these people. Vulnerable people should be vaccinated first with vaccines that are suitable for them.
This is happening everywhere in Europe as agreed, only in the Netherlands are millions of not so vulnerable people will be vaccinated before the most vulnerable will be, making itself an exception to the international ethical rules.
Previously, there has been international criticism on the exclusion of older and frail people from vaccination and treatment studies for COVID-19. These people should be the target of the vaccination, and so vaccination should be tested to see if it is effective for these people. Vulnerable people should be vaccinated first with vaccines that are suitable for them.
This is happening everywhere in Europe as agreed, only in the Netherlands are millions of not so vulnerable people will be vaccinated before the most vulnerable will be, making itself an exception to the international ethical rules.
Vaccination of the elderly
AstraZeneca provided insufficient evidence that their vaccines work well in people over 55 years and / or at risk groups. In Denmark, France, Austria, and Germany this vaccine will not be given to people over 65. In Poland not over 60 and in Italy and Belgium not over 55 years. This is a setback for the Netherlands, because most doses of the more effective vaccines had already been given to healthcare providers. Originally, the cabinet thought that 60 to 75-year-olds could be protected with AstraZeneca. Koopmans advised at an early stage to keep Pfizer for the elderly using her expert opinion (Figure 2) to make the Health Council's advice explicit.
When the EMA announced the results of the AstraZeneca trial, the Netherlands faced the dilemma of how to vaccinate the 60 to 75-year-olds. The Netherlands had vaccinated hundreds of thousands of healthcare workers with Pfizer, which could have been protected sufficiently with AstraZeneca. In a peculiar attempt of damage control, the Netherlands decided to vaccinate only people between the ages of 60 and 65 and younger people from risk groups with the AstraZeneca vaccine. The elderly people should wait for later deliveries of the RNA vaccines.
To have to wait until the end of 2021 is frustrating for the vulnerable people who have been quarantine for themselves and / or their loved one for nearly a year. They now should wait longer because of the priorities made by De Jonge. The Dutch vaccination choices imply that many elderly people will not be protected against COVID-19 until the second half of 2021. This implies that in the epidemic wave of winter 2021-2022, the Netherlands will still have many elderly people who are vulnerable to the SARS-2 virus.
When the EMA announced the results of the AstraZeneca trial, the Netherlands faced the dilemma of how to vaccinate the 60 to 75-year-olds. The Netherlands had vaccinated hundreds of thousands of healthcare workers with Pfizer, which could have been protected sufficiently with AstraZeneca. In a peculiar attempt of damage control, the Netherlands decided to vaccinate only people between the ages of 60 and 65 and younger people from risk groups with the AstraZeneca vaccine. The elderly people should wait for later deliveries of the RNA vaccines.
To have to wait until the end of 2021 is frustrating for the vulnerable people who have been quarantine for themselves and / or their loved one for nearly a year. They now should wait longer because of the priorities made by De Jonge. The Dutch vaccination choices imply that many elderly people will not be protected against COVID-19 until the second half of 2021. This implies that in the epidemic wave of winter 2021-2022, the Netherlands will still have many elderly people who are vulnerable to the SARS-2 virus.
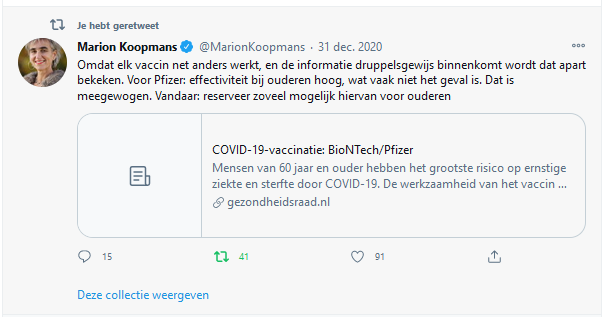
Figure 4. Koopmans explains timely why Pfizer should have been given to the elderly.
Because each vaccine works slightly differently, and the information comes in drop by drop, it is examined separately. For Pfizer: effectiveness in the elderly is high, which is often not the case. That is taken into account. Hence: reserve as much of this as possible for the elderly
Because each vaccine works slightly differently, and the information comes in drop by drop, it is examined separately. For Pfizer: effectiveness in the elderly is high, which is often not the case. That is taken into account. Hence: reserve as much of this as possible for the elderly
Vaccine roll out
All European countries have received an equal share of European vaccines in relation to their population. Belgium was ahead of their schedule but does not expect all Belgians to be vaccinated before the summer. In proportion, the Netherlands was still lags and vaccination of the high-risk groups will not be completed very soon. The Dutch procedure of vaccination is unnecessarily complex by extensive stratification of whom will be vaccinated when.
The roll-out of the vaccination is not very smooth in the Netherlands. Although we receive relatively the same deliveries than other EU countries, we are in second to last place (Figure 5). Still, nationwide vaccination campaigns are nothing new. Since 1997, risk groups in the Netherlands have been vaccinated annually against the flu. Broadly speaking, these people are those at risk for SARS-2, people over 60 or with certain medical conditions such as cardiovascular disease. Logistically this is carried out efficiently by general practitioners and for a subgroup in hospitals. With vaccination by region, this could also work for the SARS-2 vaccines.
The approach for SARS-2 is different. The GGD has selected 25 locations in the country for SARS-2 vaccination (Figure 6). However, the method seems bureaucratic and unnecessarily cumbersome, resulting in spilling of vaccines.
The roll-out of the vaccination is not very smooth in the Netherlands. Although we receive relatively the same deliveries than other EU countries, we are in second to last place (Figure 5). Still, nationwide vaccination campaigns are nothing new. Since 1997, risk groups in the Netherlands have been vaccinated annually against the flu. Broadly speaking, these people are those at risk for SARS-2, people over 60 or with certain medical conditions such as cardiovascular disease. Logistically this is carried out efficiently by general practitioners and for a subgroup in hospitals. With vaccination by region, this could also work for the SARS-2 vaccines.
The approach for SARS-2 is different. The GGD has selected 25 locations in the country for SARS-2 vaccination (Figure 6). However, the method seems bureaucratic and unnecessarily cumbersome, resulting in spilling of vaccines.
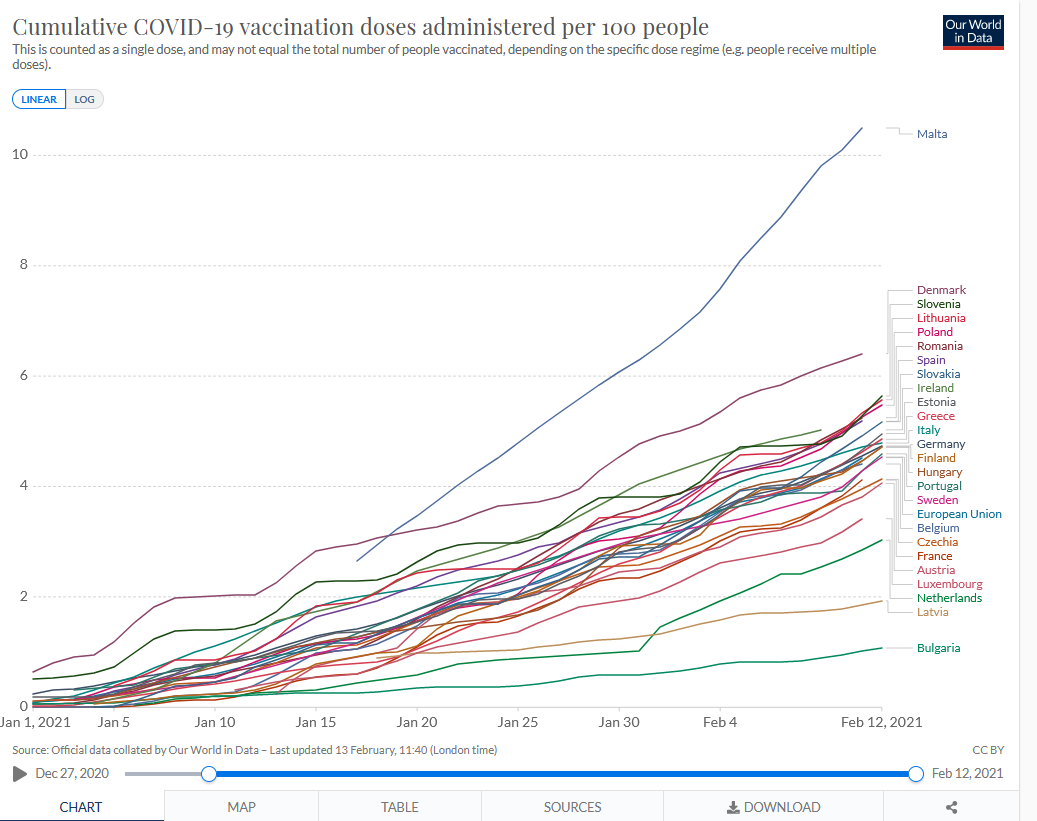
Figure 5. EU countries have jointly purchased and distributed vaccines. Nevertheless, there are differences in the progress of the vaccination campaign

Figure 6. Locations for SARS-2 vaccinations
Efficacy of vaccination in practice
Vaccination works well in people who have already had a COVID-19 infection (Figure 7). The immune response appears to mature faster.
Israel is at the frontrunner of mass vaccination in the over-60 years old. At the same time, the country imposed a lockdown to limit infections during the vaccination campaign. Immunologically, the interaction of infection and vaccination is unpredictable for a virus immune pathology.
SARS-2 vaccination reduces COVID-19 cases and hospitalizations, after the second dose (Figure 6). This effect can be seen in the vaccinated over-60s, but not in the unvaccinated young people. No ring vaccination effect cannot be seen above the lockdown effect that was also seen in places where the vaccination started a few weeks later. The strategy of the Netherlands to invest in ring vaccination therefore also appears to be ineffective in practice.
Israel is at the frontrunner of mass vaccination in the over-60 years old. At the same time, the country imposed a lockdown to limit infections during the vaccination campaign. Immunologically, the interaction of infection and vaccination is unpredictable for a virus immune pathology.
SARS-2 vaccination reduces COVID-19 cases and hospitalizations, after the second dose (Figure 6). This effect can be seen in the vaccinated over-60s, but not in the unvaccinated young people. No ring vaccination effect cannot be seen above the lockdown effect that was also seen in places where the vaccination started a few weeks later. The strategy of the Netherlands to invest in ring vaccination therefore also appears to be ineffective in practice.
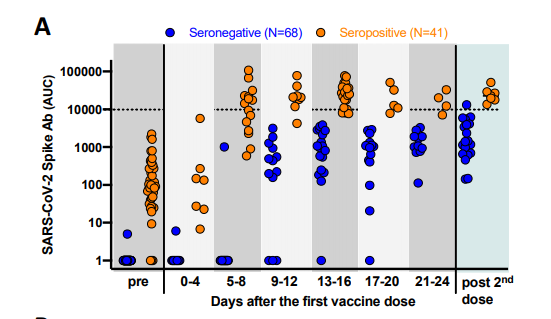
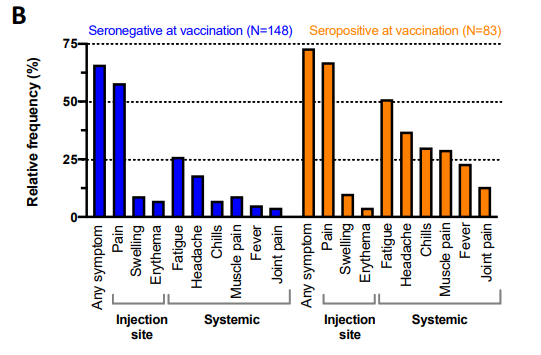
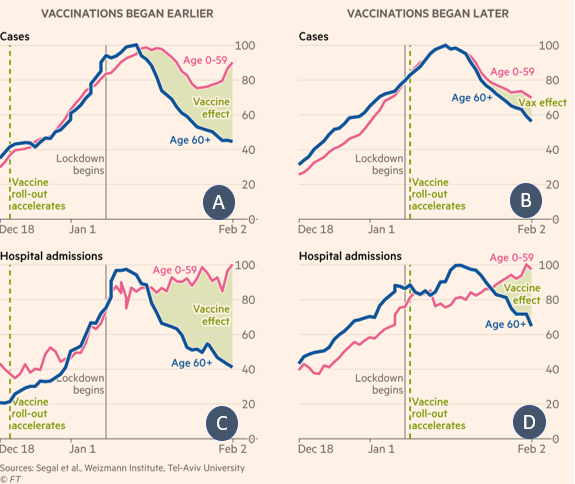
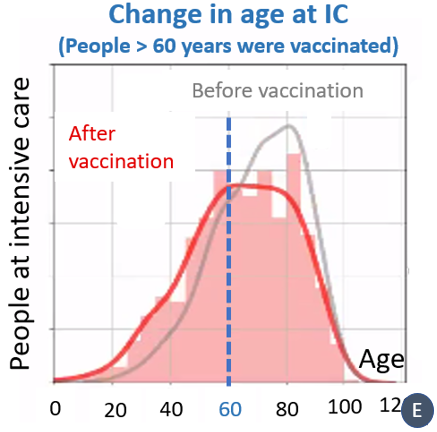
Figure 8. Development of COVID-19 cases and hospital admissions after vaccination of the over-60s in Israel.
A. Cases where vaccination started early, B cases where vaccination started later. C Hospital admissions where vaccination started early, D Hospital admissions where vaccinations started later. E. ICU admissions
A. Cases where vaccination started early, B cases where vaccination started later. C Hospital admissions where vaccination started early, D Hospital admissions where vaccinations started later. E. ICU admissions
Vaccination side effects
Just like any medical action, vaccination is not 100% safe. Any vaccine can cause anaphylactic reactions, but usually these are extremely rare, about 1 to 1,3 per 1 million injections. With the mRNA vaccines this chance is slightly higher, about 1 per 200 thousand.
In Norway, some 80-year-old people died after vaccination. Is vaccination dangerous for older people? Norway has vaccinated almost all elderly people. Normally, approximately 45 elderly die per day. There were 29 deaths the day after vaccination. Even without vaccination people die and the number was not increased.
PEG is an ingredient of most shampoos, suntan lotion and toothpaste to make them smoother, more stable or penetrate the skin better. It is also bound to pharmaceutical compounds to increase their biological availability, for example as a slow-release system. PEGs do not react chemically in the body but are sometimes recognized by the complement system (part of the natural defenses). Some people could have anaphylactic shock via IgE or directly via complement activation by PEG.
About 0.2% of people have IgE antibodies against PEG in their blood and could theoretically have an allergic reaction. If the vaccine is injected into the blood this could be dangerous for many people, however the vaccine is injected into a muscle. Then the chance that an allergy will lead to anaphylactic shock is much smaller.
The Moderna and Pfizer mRNA vaccines contain the excipient polyethylene glycol-2000 (PEG), known from shampoos, which sometimes gives an allergy reaction. The AstraZeneca vaccine contains other ingredients so could be used with a PEG allergy. Dexamethasone, a drug that is given to people in the ICU, may also contain PEG.
In Norway, some 80-year-old people died after vaccination. Is vaccination dangerous for older people? Norway has vaccinated almost all elderly people. Normally, approximately 45 elderly die per day. There were 29 deaths the day after vaccination. Even without vaccination people die and the number was not increased.
PEG is an ingredient of most shampoos, suntan lotion and toothpaste to make them smoother, more stable or penetrate the skin better. It is also bound to pharmaceutical compounds to increase their biological availability, for example as a slow-release system. PEGs do not react chemically in the body but are sometimes recognized by the complement system (part of the natural defenses). Some people could have anaphylactic shock via IgE or directly via complement activation by PEG.
About 0.2% of people have IgE antibodies against PEG in their blood and could theoretically have an allergic reaction. If the vaccine is injected into the blood this could be dangerous for many people, however the vaccine is injected into a muscle. Then the chance that an allergy will lead to anaphylactic shock is much smaller.
The Moderna and Pfizer mRNA vaccines contain the excipient polyethylene glycol-2000 (PEG), known from shampoos, which sometimes gives an allergy reaction. The AstraZeneca vaccine contains other ingredients so could be used with a PEG allergy. Dexamethasone, a drug that is given to people in the ICU, may also contain PEG.
Batch to batch variation
Vaccine production is complex technology that we can implement but may yield variable results between batches. From my early career, when I was doing R&D of vaccine production, I know that purchased batches can lead to large differences in yield and quality. This also applies to other vaccines, such as the virus production or the vaccines by AstraZeneca and Janssen.
For Pfizer, these are differences in the purity of the active substance: vaccines in the trials had 78% intact RNA, vaccines for large-scale vaccination only 55%. Having lead vaccine production R&D, I am not surprised by these differences between batches. Generating consistent high quality in high-tech production involves many challenges. It also implies that while the vaccines are rated safe, every batch should be still monitored for unexpected behaviour and efficacy.
For Pfizer, these are differences in the purity of the active substance: vaccines in the trials had 78% intact RNA, vaccines for large-scale vaccination only 55%. Having lead vaccine production R&D, I am not surprised by these differences between batches. Generating consistent high quality in high-tech production involves many challenges. It also implies that while the vaccines are rated safe, every batch should be still monitored for unexpected behaviour and efficacy.
Limited sterilizing immunity after vaccination
Copying Koopmans, Van Dissel states that sterilizing immunity after vaccination is unlikely for respiratory viruses. Vaccination produces good IgG antibodies, but only in a small proportion and often little IgA (Figure 8). At Moderna, about half have IgA and only a few at Pfizer. Immunologists expect that IgA is required for sterilizing immunity. Vaccines therefore seem to protect well against disease, but not against infection. The Moderna vaccine may provide ~ 50% protection against infection. For a ring vaccination or group immunity, this is completely insufficient to prevent the virus from entering healthcare institutions. The ring vaccination is therefore not an effective method to protect people.
AstraZeneca showed that vaccination decreased disease but did not change asymptomatic infections. This suggests that fewer people would be infected. It is difficult to estimate how the impact on the spread will be, since diseased people are unlikely to be super spreaders, as they generally withdraw from crowds. It should be noted that this study follow-up until 4 months after vaccination (while omitting the first month). Currently, there are no indications that sterilizing immunity would be better after regular vaccination than after infection.
Despite all the evidence against sterilizing immunity, the Dutch government continues to communicate that vaccination is important to protect others around you (Figure 10; Figure 11). This is not claimed by the manufacturer, the EMA, the MEB and the RIVM. If people believe this lie it could cause them to infect others by uncareful behaviour.
AstraZeneca showed that vaccination decreased disease but did not change asymptomatic infections. This suggests that fewer people would be infected. It is difficult to estimate how the impact on the spread will be, since diseased people are unlikely to be super spreaders, as they generally withdraw from crowds. It should be noted that this study follow-up until 4 months after vaccination (while omitting the first month). Currently, there are no indications that sterilizing immunity would be better after regular vaccination than after infection.
Despite all the evidence against sterilizing immunity, the Dutch government continues to communicate that vaccination is important to protect others around you (Figure 10; Figure 11). This is not claimed by the manufacturer, the EMA, the MEB and the RIVM. If people believe this lie it could cause them to infect others by uncareful behaviour.
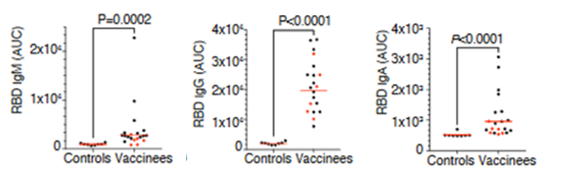
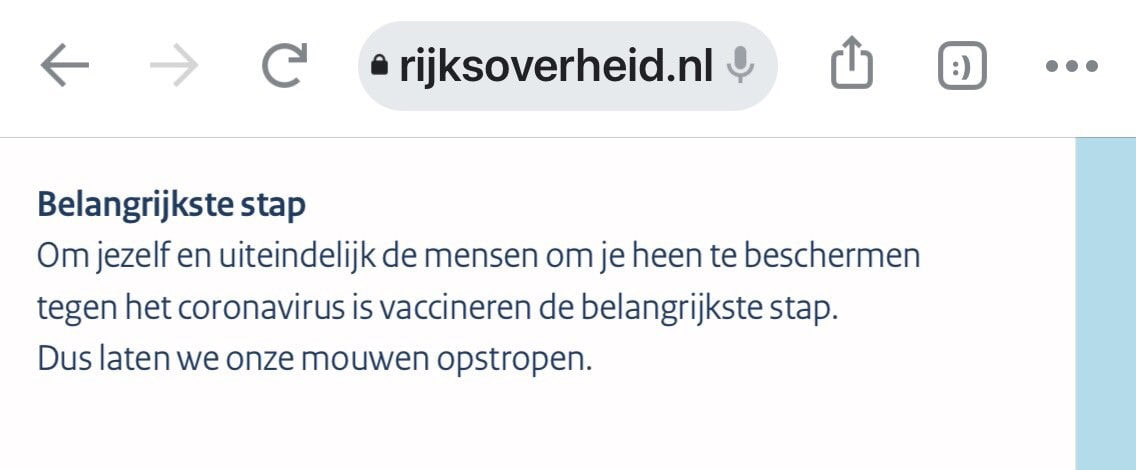
Figure 10. Dutch advertising about vaccination.
Top “Vaccination is the most important step to protect yourself and the people surrounding you against the coronavirus” Right “I want the vaccin because I see so many people suffering at the Covid department. I hope to reduce the number of infections in this way.” |

|

Figure 11. Response to vaccination poster.
Stop spreading misinformation! It is still not clear that vaccination protects others, that it prevents contagiousness. Your FAQ is also incorrect, because the answer is about getting sick and not about contagiousness.
Stop spreading misinformation! It is still not clear that vaccination protects others, that it prevents contagiousness. Your FAQ is also incorrect, because the answer is about getting sick and not about contagiousness.
Limited protection against mutants after vaccination.
The neutralizing antibodies induced by vaccination were tested for their effectiveness against mutants. In 14 of the 17 most potent antibodies, neutralization was reduced or gone due to mutations at 1 amino acid. We also know mutants with multiple changes. So the chance that escape mutants will break through after vaccination is real.
The odds are worse for people who have only received one out of two injections. Nevertheless, the Dutch government postpone the period between the first and second injection from three to six weeks. Experts are concerned about this because people will be partially protected for a prolonged period. The data from the natural infection show that maturation of antibodies is important for a good defence against mutants. Ironically, the cabinet is motivating this with more people being protected from the British mutant. Anyone with knowledge of the evolution of escape mutants knows that the best way to get them is partially effective strategy, be it half a course of antibiotics against bacteria or half a vaccination with immature antibodies against a virus infection. Resistance to the vaccine is the last thing you should want. The EMA has clarified its advice and explicitly set it at three weeks.
The odds are worse for people who have only received one out of two injections. Nevertheless, the Dutch government postpone the period between the first and second injection from three to six weeks. Experts are concerned about this because people will be partially protected for a prolonged period. The data from the natural infection show that maturation of antibodies is important for a good defence against mutants. Ironically, the cabinet is motivating this with more people being protected from the British mutant. Anyone with knowledge of the evolution of escape mutants knows that the best way to get them is partially effective strategy, be it half a course of antibiotics against bacteria or half a vaccination with immature antibodies against a virus infection. Resistance to the vaccine is the last thing you should want. The EMA has clarified its advice and explicitly set it at three weeks.
Virus Ethics
Effective and open
Do we strife for the good things?
Beyond mortality
Special immunity
Vaccination
Prevention of epidemic
Effective and open
Do we strife for the good things?
Beyond mortality
Special immunity
Vaccination
Prevention of epidemic
