COVID-19
Two years COVID-19:Looking back and forward
III. Morbid tales
Morbidity after COVID-19 might cause more loss of quality-adjusted life years (QALYs) than mortality due to acute COVID-19. A physician stated “There’s mounting evidence that the hospitalizations and deaths that result from the acute phase of COVID-19 are only the tip of the iceberg. I strongly suspect that countries that allow the virus to spread will experience a larger, secondary epidemic of chronic disease.” [T] The WHO estimates infection-mortality rates to be approximately 0.5 - 1%.[WHO], with probably somewhat higher numbers for Western countries, related to their population age distribution.[JJ]
Underlying conditions
“If you’re young and healthy, death from COVID may be highly unlikely, but severe debilitation is not”, according to Putrino.[Ledford] The severity of a disease is measured by its mortality rate but provides an incomplete picture. A long list of underlying illnesses have been defined, including diabetes, lung disease, cancer, immunodeficiency, heart disease, hypertension, asthma, kidney disease, gastrointestinal and liver disease, and obesity.[NYC] Others might add pregnancy and smoking to this list.[UMMS] In case of pregnancy, risks of severe outcomes are both for mother and child, especially in the last three months.[UU] Mortality rates for COVID-19 are higher for the elderly, with postulations that this may be due to correlations with the greater likelihood of these individuals suffering from underlying risk factors.
Underlying risk factors are crucial for personalized medicine i.e., these risk factors are identified for personal prevention of disease, like cardiovascular disease on U-Prevent. It is invaluable for personal risk management but should not be confused with people being (nearly) moribund. Many people dying of COVID-19, still had a good life expectancy would they not have died i.e., the average years of life lost per death is 16 years.[Pifarré i Arolas] General mortality rates have a similar distribution and from the beginning of the epidemic it is known that at any age or medical condition a relevant number of people die from SARS-2. Playing the epidemic down to only the elderly would die violates both ethical principles and relative mortality numbers per age group.
SARS-2 infection during pregnancy can be dangerous at any time, but this risk to both the mother and fetus, as well as placental damage, increases during the third trimester. [Arthurs]
Underlying risk factors are crucial for personalized medicine i.e., these risk factors are identified for personal prevention of disease, like cardiovascular disease on U-Prevent. It is invaluable for personal risk management but should not be confused with people being (nearly) moribund. Many people dying of COVID-19, still had a good life expectancy would they not have died i.e., the average years of life lost per death is 16 years.[Pifarré i Arolas] General mortality rates have a similar distribution and from the beginning of the epidemic it is known that at any age or medical condition a relevant number of people die from SARS-2. Playing the epidemic down to only the elderly would die violates both ethical principles and relative mortality numbers per age group.
SARS-2 infection during pregnancy can be dangerous at any time, but this risk to both the mother and fetus, as well as placental damage, increases during the third trimester. [Arthurs]
Acute disease: COVID-19
Acute SARS-2 infection could cause lung disease, brain disease, sepsis-like syndrome destroying the immune system and disseminated thrombosis. SARS-2, like many other diseases, doesn’t only kill people, also many people have prolonged disease (long covid) and various morbidities [JJ]:
Severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) can trigger a cytokine storm in the pulmonary tissue by releasing various types of mediators, leading to acute respiratory distress syndrome (ARDS). Increased neutrophil‐to‐lymphocyte ratio, as well as CD4+ T lymphopenia, is reported in cases with novel coronavirus disease (COVID‐19), meanwhile, lymphopenia is a significant finding in the majority of COVID‐19 cases with a severe phenotype. Moreover, excessive activation of monocyte/macrophage and cytokine storms are associated with the severity of the disease and the related complications in SARS‐CoV‐2 infection. [Mohamed Khosroshahi]
- Brain infection by SARS-2 through the Neuropilin-1 receptor [Cantuti-Castelvetri]. SARS-2 infections destroys brain centers involved in taste and smell but also many other symptoms are observed e.g., brain fog but also more serious complaints. Spike is the major determinant of pathogenesis. [Cowley,Philips]
- Destruction of lung tissue, especially the capillaries involved in oxygen uptake. This leads to prolonged feeling reduced oxygen saturation in blood and tiredness.
- Systemic infection by cell entry through ACE2 which is present in almost every tissue for oxygen regulation (Figure 1). This could lead to the multi inflammatory syndrome but also to thrombosis or direct dispersed tissue damage (Figure 2).
- SARS-2 infections undermines the immune system through various mechanisms. When the SARS-2 virus infects B-lymphocytes, the spike protein could be relocated to the nucleus and interfere with the process of antibody maturation.[JJ] This might be a molecular mechanism by which SARS-2 selectively inhibits antigen-specific immunity.[Jiang] The virus also inhibits cellular immunity, like T lymphocytes[Qin] and NK cells. Posttreatment decreases in CD8+ T cells and B cells and increase in CD4+/CD8+ ratio were indicated as independent predictors of poor efficacy. [Wang]
- SARS-2 infections can persist in the body, leading to prolonged symptoms.[Zapor, Jacobs21]
Severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) can trigger a cytokine storm in the pulmonary tissue by releasing various types of mediators, leading to acute respiratory distress syndrome (ARDS). Increased neutrophil‐to‐lymphocyte ratio, as well as CD4+ T lymphopenia, is reported in cases with novel coronavirus disease (COVID‐19), meanwhile, lymphopenia is a significant finding in the majority of COVID‐19 cases with a severe phenotype. Moreover, excessive activation of monocyte/macrophage and cytokine storms are associated with the severity of the disease and the related complications in SARS‐CoV‐2 infection. [Mohamed Khosroshahi]
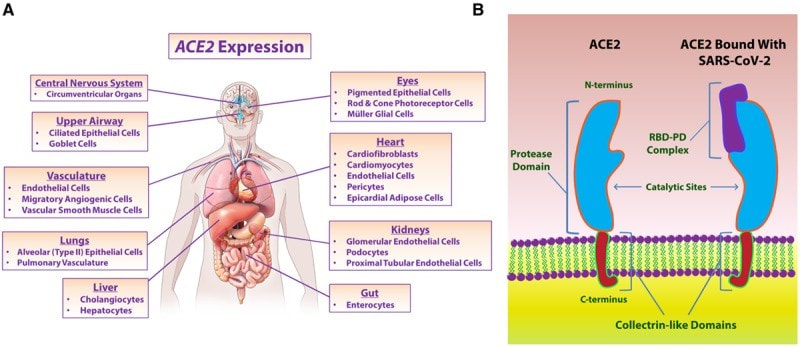
Figure 1. Distrubtion of ACE2 in the body [Gheblawi]
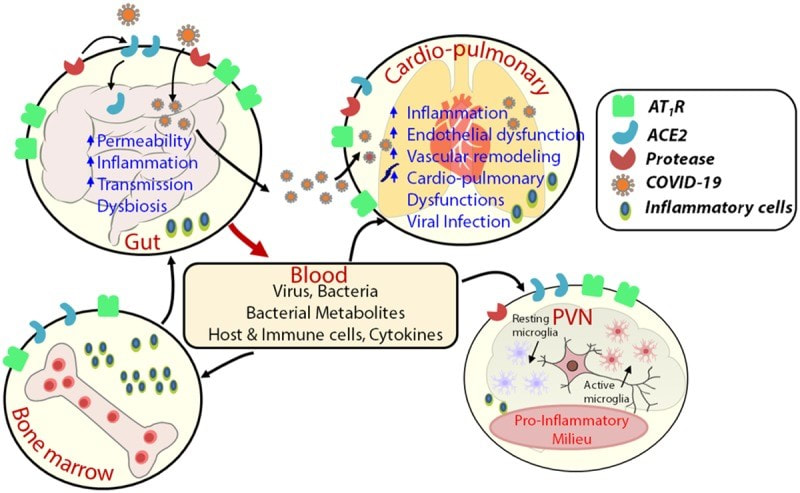
Figure 2. Effects of SARS-2 related to ACE2[Gheblawi]
Long covid
Long covid does not have the same risk factors than acute COVID but appears to affect the apparent healthy people. Long covid does not appear to be age restricted, is more prone in female, and seems unrelated to other pre-diagnostic comorbidities. [Mohamed-Hussein] Over 100 symptoms have been listed, and the disease is multisystemic. [Hayes. Suvvari, Desai] The symptoms of Long covid differ strongly from the acute phase (Figure 3). In November 2021, I presented some results from the P4O2 consortium at a long covid conference. Younger people often report long covid complaints,[T, Estiri]. A variety of complaints have been reviewed [JJ] (Figure 4)(Figure 5):
Hypothetical mechanisms
At a long-covid conference in November 2021, I listed some putative mechanisms of this disease:
Most likely different groups of long-covid patients will have different diseases, and some will have combinations hereof. One to five are immunological diseases related to the superantigen and SARS-2 pro-inflammatory properties. A short corticosteroid course reduces symptoms and immunological alterations underlying long-COVID. [Utrero-Rico]
- Olfactory disorders persisted at least one year after COVID-19 – smell problems were frequent (5% anosmia, 22% hyposmia) versus only 3.5% hyposmia in the control group) .[Vaira]
- Various neurological symptoms, including brain fog. [Williams, Asadi-Pooya]
- Reduced brain metabolism (Figure 6).[Guedj]
- Cardiovascular disease including thrombosis, pericarditis [Carubbi] and insufficient ACE2 signaling from various tissues for call for increased circulation.
- Pulmonological disease due to damage of small blood vessels
- Various long covid complaints,[Lutchmansingh] including tiredness and diabetes,[Caruso, Feldman, Lima-Martínez, Buttery, Di Toro, Lund]
- Local and systemic immune activation indicated by proinflammatory cytokines.[Schultheiß, Kappelman, De Winter, Peluso]
- Dysregulation of antigen specific immunity, indicated by deficiencies in Dendritic cells [Pérez-Gómez], altered B-cell [Peghin] and T-cell functions.[Cheon,Glynne, Roe] Similar immunological changes are also seen in cancer and AIDS, indicating that severe long-covid could become a major health problem.
Hypothetical mechanisms
At a long-covid conference in November 2021, I listed some putative mechanisms of this disease:
- Continued inflammation by immune dysregulation.
- Persistent SARS-2 infection, immune exacerbations by triggered by superantigen. [Jacobs21] At least 6 months of brain infection has been shown in people with anosmia.[Dias de Melo]
- Induction of disease by other viruses, like the herpesviruses EBV and CMV. [Gold]
- Cardiovascular infarcts due to thrombosis.
- Auto-immunity like Anti-idiotype antibodies in SARS-CoV-2 [Murphy].
- Neurological damage related to brain infection [Benedetti, Yong] through the Neuropilin 1 receptor [Abebe].
- SARS-2 causes Lewy body formation which is an indication for the development of Parkison’s disease in humans. [Philippens]
- Neurological infections by other coronaviruses have been suggested in the pathogenesis of multiple sclerosis and other demyelinating diseases [Gallagher, Wege, Owens, Talbot, Cabirac, Collins, Haring, Murray and now also for SARS-2. [Rogers, Bellucci]
- Psychological effect due to severe infection in combination with other disease effects.
Most likely different groups of long-covid patients will have different diseases, and some will have combinations hereof. One to five are immunological diseases related to the superantigen and SARS-2 pro-inflammatory properties. A short corticosteroid course reduces symptoms and immunological alterations underlying long-COVID. [Utrero-Rico]
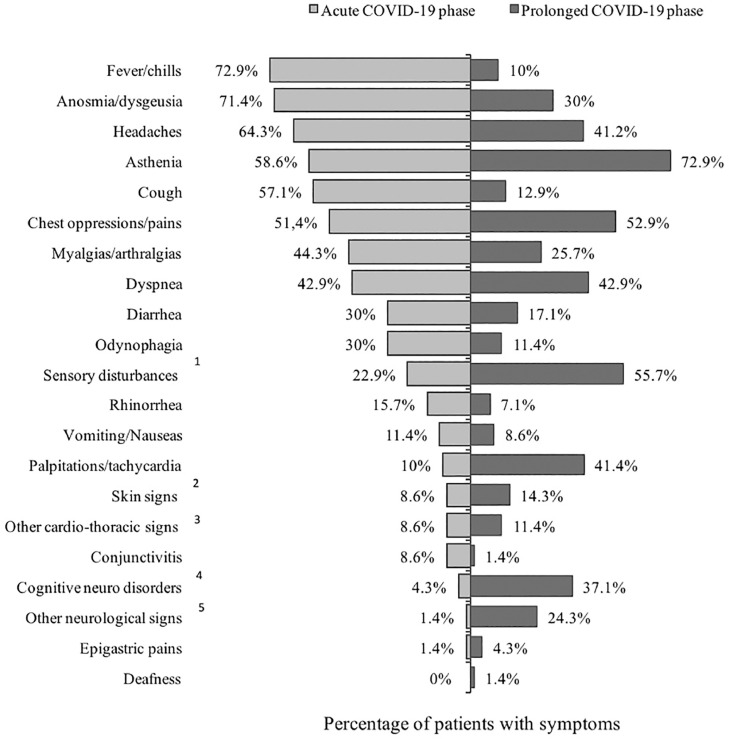
Figure 3. Symptoms in acute and long covid [Salmon-Ceron]
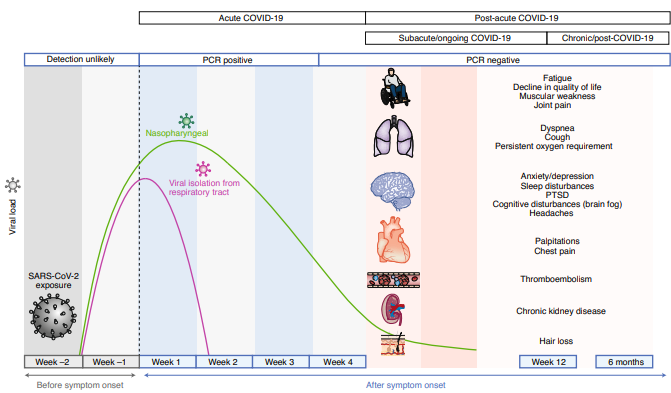
Figure 4. Long COVID symptoms become noticed 3 to 6 months after infection.[Davis]
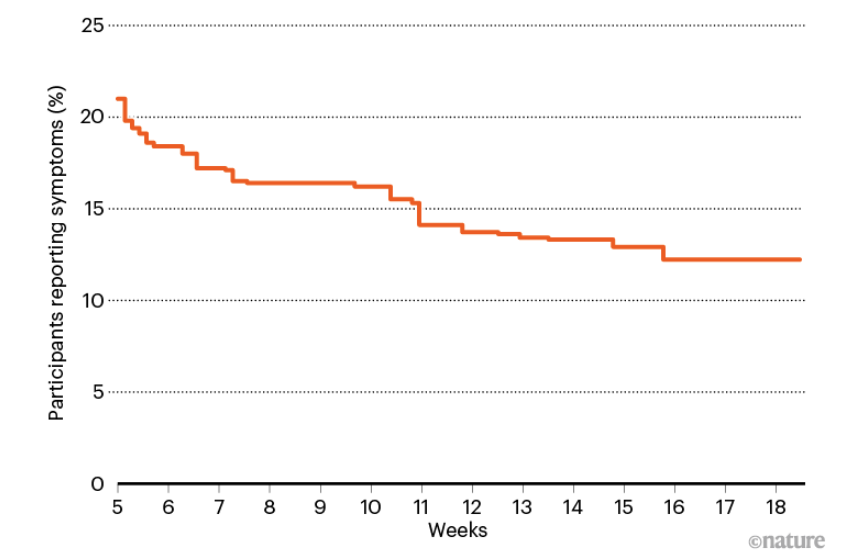
Figure 5. Long covid symptoms slowly disappear [Marshall]
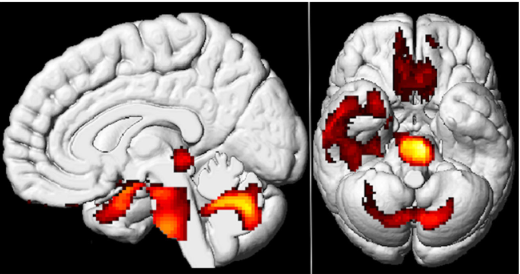
Figure 6. Areas of decreased brain metabolism in long covid.[Guedj]
Children
The research on COVID-19 in children started very late, due to the false belief that children were not affected and not important for understanding the dynamics of the pandemic, stated Giaquinto. “It is extremely important that we eventually recognize the key role that children and adolescents play in the epidemic and the natural history of childhood infection, with particular reference to the long-term consequences of the infection.[Verdi project]
Mortality rate of children due to SARS-2 is 0.005% (50/1million infections) in the UK, with a threefold higher number dying with a SARS-2 infection [Smith]. A larger number of children suffer from chronic disease after SARS-2. A pediatrician stated that COVID-19 is one of the most serious childhood disease.[Zwiauer] According to the CDC, young children, are at risk for severe COVID-19 (Figure 7).[CDC] In one and a halve year, 2 million 5- to 11-year-olds have gotten ill from COVID-19, and 94 have died in the USA.[ME] Similar numbers are reported from other countries.[NL,SE] In the Netherlands, ~50 children were admitted to the ICU,[NOS] and 9 children have died.[Mooy] At population level, children seem to have similar risks for most COVID-19 symptoms, albeit les for pulmonary symptoms and more for thrombosis. [Roessler]
Children are at risk for neurological complication of COVID-19.[Lindan] Nearly all children hospitalized with SARS-2 infection had markers of thrombotic microangiopathy (TMA), clothing inside small blood vessels e.g., thrombocytopenia, anemia, and purpura (purple skin spots). They also often have markers of complement activation which is associated with renal dysfunction.[Diorio, Al-Ghafry] Studies are investigating if type 1 diabetes in children is caused by COVID-19.[Unsworth]
Very few children are likely to develop severe disease [Rathore] Multi-inflammatory syndrome in children (MIS-C) is a relative frequent life-threatening complication for previously healthy children after covid.[Ahmed, Panigrahy. Feldstein, García-Salido] MIS-C develops 4-6 weeks following SARS-CoV-2 infection, and is presumably initiated by adaptive immune response. Though it has multisystem involvement, it is the cardiovascular manifestations that are most prominent. High titres of anti-SARS-CoV-2 antibodies are seen in these patients. As this is a new disease entity, its immunopathogenesis is not fully elucidated.[Kabeerdoss]. MIS-C might be caused by SARS-2’s superantigen,[NG] which might be also responsible for persistent infection and long COVID. [Jacobs21]
COVID-19-related mortality and morbidity is the reason why some countries, after safety studies,[ME] authorized vaccines for children age 5 to 11 years old at ⅓ of the adult dose.[USA, CA; IL] The EMA has a vaccine approved for children, so children may be protected safely by vaccinaton.[Van Gool] Containment Now calls to protect children by vaccination.
School closures are heavily debated but not always with appropriate arguments. Children living in unsafe homes also need protection beyond the hours at school, lack of food is a valid argument in the Third world but not in Western countries. Comparing stress before and during the epidemic is not a honest comparison, and strategic motives may sometimes play a role (V).
Online classes over physical education might limit virus spread in children but only where affordable. School closures might not be ideal as a sustained, primary intervention for controlling COVID-19,[Wu] since prolonged school closures do have some consequences.[UNESCO] Testing, vaccination, facemasks and other antiviral strategies might allow prolonged physical education.
Mortality rate of children due to SARS-2 is 0.005% (50/1million infections) in the UK, with a threefold higher number dying with a SARS-2 infection [Smith]. A larger number of children suffer from chronic disease after SARS-2. A pediatrician stated that COVID-19 is one of the most serious childhood disease.[Zwiauer] According to the CDC, young children, are at risk for severe COVID-19 (Figure 7).[CDC] In one and a halve year, 2 million 5- to 11-year-olds have gotten ill from COVID-19, and 94 have died in the USA.[ME] Similar numbers are reported from other countries.[NL,SE] In the Netherlands, ~50 children were admitted to the ICU,[NOS] and 9 children have died.[Mooy] At population level, children seem to have similar risks for most COVID-19 symptoms, albeit les for pulmonary symptoms and more for thrombosis. [Roessler]
Children are at risk for neurological complication of COVID-19.[Lindan] Nearly all children hospitalized with SARS-2 infection had markers of thrombotic microangiopathy (TMA), clothing inside small blood vessels e.g., thrombocytopenia, anemia, and purpura (purple skin spots). They also often have markers of complement activation which is associated with renal dysfunction.[Diorio, Al-Ghafry] Studies are investigating if type 1 diabetes in children is caused by COVID-19.[Unsworth]
Very few children are likely to develop severe disease [Rathore] Multi-inflammatory syndrome in children (MIS-C) is a relative frequent life-threatening complication for previously healthy children after covid.[Ahmed, Panigrahy. Feldstein, García-Salido] MIS-C develops 4-6 weeks following SARS-CoV-2 infection, and is presumably initiated by adaptive immune response. Though it has multisystem involvement, it is the cardiovascular manifestations that are most prominent. High titres of anti-SARS-CoV-2 antibodies are seen in these patients. As this is a new disease entity, its immunopathogenesis is not fully elucidated.[Kabeerdoss]. MIS-C might be caused by SARS-2’s superantigen,[NG] which might be also responsible for persistent infection and long COVID. [Jacobs21]
COVID-19-related mortality and morbidity is the reason why some countries, after safety studies,[ME] authorized vaccines for children age 5 to 11 years old at ⅓ of the adult dose.[USA, CA; IL] The EMA has a vaccine approved for children, so children may be protected safely by vaccinaton.[Van Gool] Containment Now calls to protect children by vaccination.
School closures are heavily debated but not always with appropriate arguments. Children living in unsafe homes also need protection beyond the hours at school, lack of food is a valid argument in the Third world but not in Western countries. Comparing stress before and during the epidemic is not a honest comparison, and strategic motives may sometimes play a role (V).
Online classes over physical education might limit virus spread in children but only where affordable. School closures might not be ideal as a sustained, primary intervention for controlling COVID-19,[Wu] since prolonged school closures do have some consequences.[UNESCO] Testing, vaccination, facemasks and other antiviral strategies might allow prolonged physical education.
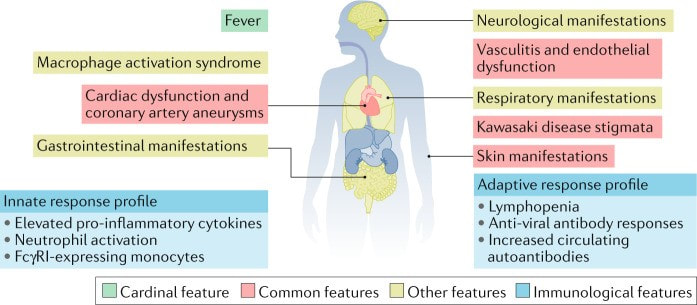
Figure 7. Emerging clinical and immunological features of MIS-C. [Henderson]
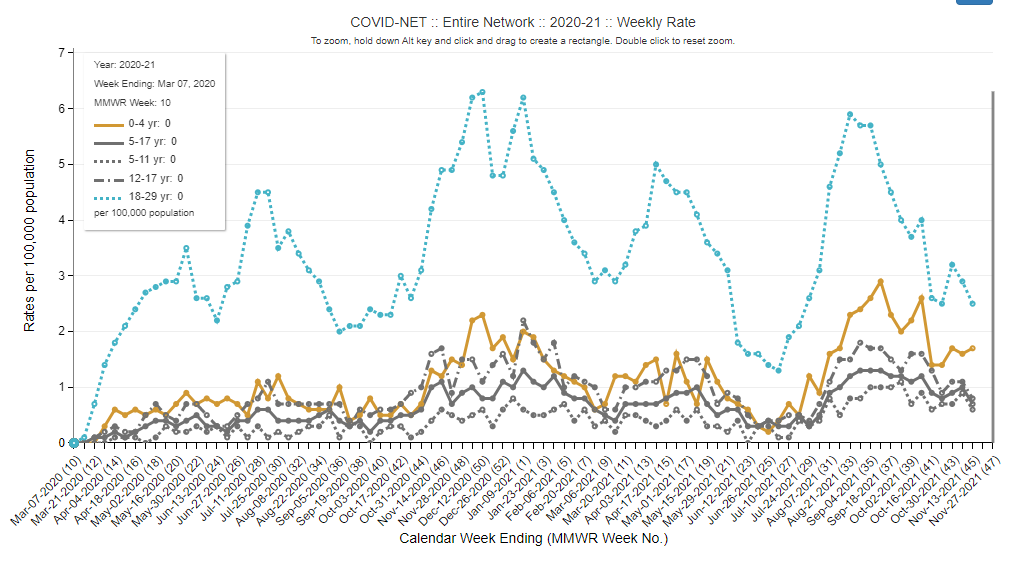
Figure 8. Hospitalization of young people with COVID-19 in the USA. [CDC]
Africa is hit hard
The shortage of vaccines in Africa is huge.[WHO] COVID-19 is rapidly increasing in Africa with more virulent SARS-2 variants.[WHO] Since most African countries have less people with cardiovascular disease i.e., underlying conditions, the mortality rate should have been much lower.[Lawal] Inadequate treatment for critically ill patients contributed to higher death rates in Africa, compared to other parts of the world.[NYT] About 19% of the deaths in Africa was associated with SARS-2 infection, and ¾ were aged under 60 years. [Mwananyanda,Kirenga]
The severity of the epidemic in Africa raises a few points.
The severity of the epidemic in Africa raises a few points.
- Firstly compassion to people suffering.
- Secondly, even a young population is severely affected, COVID-19 is not a disease of the elderly.
- Thirdly, it illustrates that SARS-2 left untreated is devastating for society.
- Fourthly, fighting COVID-19 requires strong medical support.
- Finally, fighting the epidemic will be extremely costly.
|
|
|
