COVID-19
Prevent contamination
John Jacobs, 6th March 2021.
Understanding exponential functions is crucial in virus epidemiology. Intuitively, people find exponential functions difficult. People who do not understand exponential function think of solution that will not work in practice and lead to a lot of misery. The classical chessboard explains it starting with 1 grain of rice on the first square of a chessboard, 2 on the second, 4 on the third. 8 on the fourth and so the doubling continues until the world cannot contain all the rice. This cannot be continued so it should be stopped at some time. The natural ending implies that the maximum number of victims that the epidemic could achieve has been reached - not exactly a noble endeavor. The epidemic of a viral disease can have two natural ends. First everyone is immune to the disease and second herd immunity. A
Vaccination is ineffective in fighting the epidemic. Before and / or at the onset of symptoms, people have the highest virus titres in the throat and nasal cavity and people are the most contagious. Because vaccination does little to reduce infectiousness, a vaccination certificate is of little use to fight the disease spreading. It is important that infected people are identified. The RT-PCR can do this, is very sensitive – even more than required, and takes a lot of time. Given the wide differences in virus titers, it is important to test daily (Figure 1). Rapid tests can offer a solution.
- Everyone is immune means that no one will have the disease anymore. If and when this will be would depend on how long people remain protected after infection or vaccination and whether escape mutants arise. We do not know how long immunity remains after SARS-2 infection and / or vaccination. Shortly after infection or vaccination, about 95% are immune, but immunity wanes in time. The decrease is clear but seems to be slower than with the corona cold viruses, where protection is lost after 6 months on average. It is realistic to assume that people should be vaccinated every year or every other year. The high virus circulation in major parts of the world, generates mutants that evade the immune response. That could cause a new epidemic of SARS-2.1 or SARS-3, i.e., viruses to which people are only partially or not at all immune.
- Herd immunity assumes that after infection or vaccination, a high percentage of people and their subgroups will yield sterilizing immunity. When exactly herd immunity is achieved depends on the R0. Before the start of the lockdown measures it was R0 ~ 4, later it fell. If R0 = 3 then 1-⅓ = 67% must have sterilizing immunity, for R0-4 then 75%, to stop the epidemic completely. In Manaus, 76% had signs of immunity but this was insufficient for a measurable effect on new infection, showing that it was not even close to herd immunity. Respiratory viruses generally do not yield lasting sterilizing immunity. Virologists and immunologists differentiate between sterilizing and non-sterilizing immunity. Both protect against disease but the first also against infection. For most bacteria and viruses, protection against infection and disease is caused by IgG antibodies and T cells. Immunity in the gastrointestinal tract and of the upper respiratory tract is different. These pathogens, like coronaviruses, can only be fully eliminated by IgA-mediated sterilizing immunity. Immunologists think that IgA is required for sterilizing immunity. IgA is produced between months 1 and 3 after infection or vaccination in ⅔ to ¾ of the people. Studies for sterilizing immunity within three months after vaccination may give some promising results, but the presumed mechanism is later disappearing. In addition, herd immunity requires sufficient immunity in each target group. In the case of polio, RIVM is concerned about the loss of protection among in reformed communities where protection is too low. If the vaccination protocols would be complete and yielded good sterilizing immunity children under the age of 18 could still be contagious since these would be unvaccinated.
- An an everlasting epidemic like the four coronaviruses causing the common cold. An epidemic ends only if one of these conditions is met, long-lasting immunity against the disease develops or the disease is permanently eradicated. Considering the immunity in other coronaviruses and what we see with COVID-19, it is very unlikely that lasting immunity will develop. The implication could be that this epidemic would be never ending, like the corona common cold virus, albeit a worse disease. So far there are no indication that the COVID1-9 become less virulent, only contraindications (see section “Mutants” at the end). Limiting virus spread and impact seem to be the only sustainable strategies.
Vaccination is ineffective in fighting the epidemic. Before and / or at the onset of symptoms, people have the highest virus titres in the throat and nasal cavity and people are the most contagious. Because vaccination does little to reduce infectiousness, a vaccination certificate is of little use to fight the disease spreading. It is important that infected people are identified. The RT-PCR can do this, is very sensitive – even more than required, and takes a lot of time. Given the wide differences in virus titers, it is important to test daily (Figure 1). Rapid tests can offer a solution.
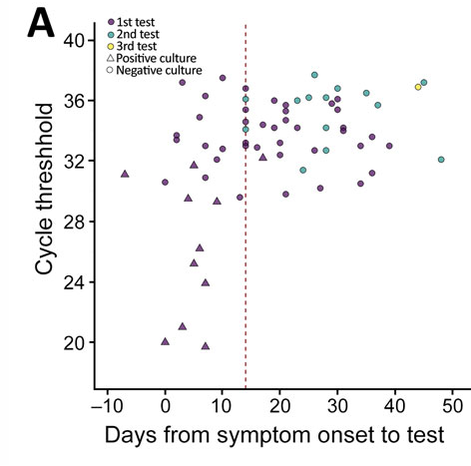
Figure 1. Number of RT-PCR cycles required to detect virus at different times after the onset of symptoms.
Lower cycle count means more virus RNA in a sample. Virus can almost always be grown on samples of up to 30 cycles
Lower cycle count means more virus RNA in a sample. Virus can almost always be grown on samples of up to 30 cycles
Reduce or increase infections?
Do you want to reduce or increase virus infections and disease? Given the impact and ethics of the developments, it is not inconceivable that a future trial will evaluate our ethical choices. Some countries, consciously or unconsciously, aim to increase virus infections, others to decrease. Although the modelling is complex, countries that increase virus infections have more morbidity and mortality and no detectable herd immunity. It was falsely suggested by 44-52% of seropositive people but rapidly disproven when 75% was infected and still rising. Europe and America fail to control the epidemic. Countries in East Asia and Australia have moved, except for sporadic cases, beyond the epidemic for already six months. Comparing mortality rates between countries may be complicated, it is obvious that mortality rates in South Korea, Thailand, and Vietnam are much lower than Brazil, the UK, and the US.
SARS-2 has infected 116 million people, causing 2.6 million deaths, worldwide. That means that now about 1.5% of the world was diagnosed with COVID-19, 0,33‰ of people have died of the disease, which is, 2,2% of the cases. The increases in cases and mortality of 35% and 38% in the last two months do not suggest that the epidemic is nearly over – in spite of all vaccination efforts in 2021. Globally, death from COVID-19 has a strong correlation with the reported SARS-2 cases, despite the ever-changing definition of a case, differences in population age distribution and health care (Figure 2). The correlations before and after adjustment for population are extremely good (R ^ 2 = 0.92 and 0.89).
In the Netherlands and Belgium, 10 to 15% of people have been infected with SARS-2, which is a factor of 30 to 50 higher than in East Asia and Australia (Figure 3). There are also large differences between neighbouring countries within Europe. Germany fights the virus more effectively than its neighbours, the Netherlands and Belgium, and Germany has about half the mortality of its neighbours. Conversely, Sweden fights less effectively and has about 10 times higher mortality than the two neighbouring countries Norway and Finland.
SARS-2 has infected 116 million people, causing 2.6 million deaths, worldwide. That means that now about 1.5% of the world was diagnosed with COVID-19, 0,33‰ of people have died of the disease, which is, 2,2% of the cases. The increases in cases and mortality of 35% and 38% in the last two months do not suggest that the epidemic is nearly over – in spite of all vaccination efforts in 2021. Globally, death from COVID-19 has a strong correlation with the reported SARS-2 cases, despite the ever-changing definition of a case, differences in population age distribution and health care (Figure 2). The correlations before and after adjustment for population are extremely good (R ^ 2 = 0.92 and 0.89).
In the Netherlands and Belgium, 10 to 15% of people have been infected with SARS-2, which is a factor of 30 to 50 higher than in East Asia and Australia (Figure 3). There are also large differences between neighbouring countries within Europe. Germany fights the virus more effectively than its neighbours, the Netherlands and Belgium, and Germany has about half the mortality of its neighbours. Conversely, Sweden fights less effectively and has about 10 times higher mortality than the two neighbouring countries Norway and Finland.
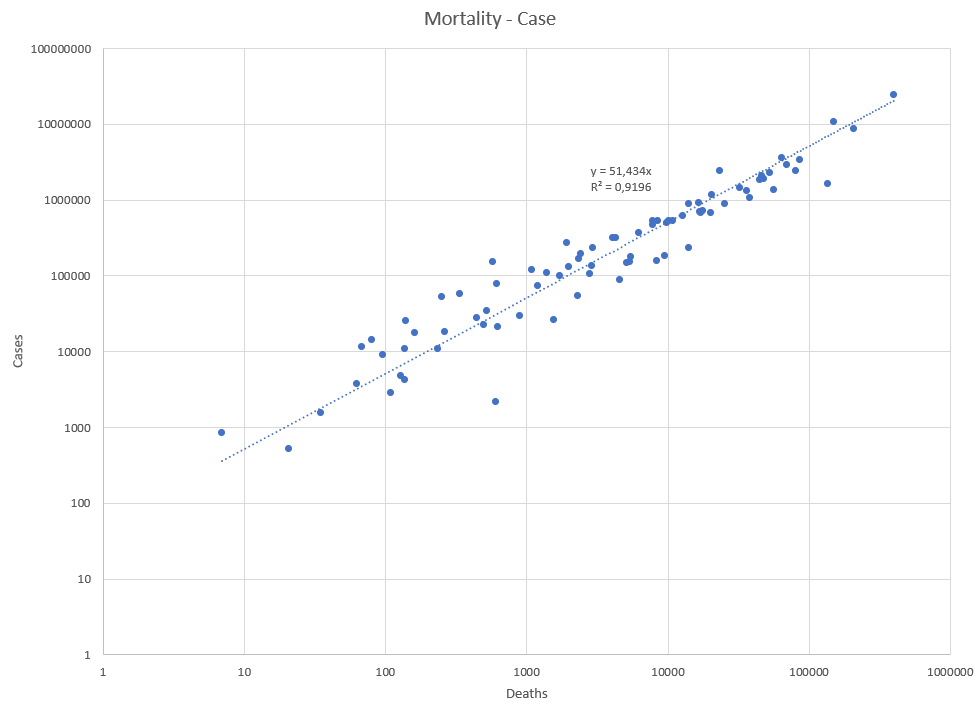
Figure 2. Relationship between number of cases and mortality from SARS-2
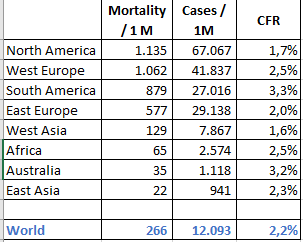
Figure 3. Mortality and number of cases per continent.
Medical is not epidemiological.
SARS-2 infection in the oral and nasal cavity is related to infecting other people but infection in the lungs or in the bloodstream could cause serious or fatal disease. Many people, including some physicians, have trouble to understand the difference between medical treatment of disease and fighting the epidemic. This confuses the discussion and could result in incorrect advices.
Medical care is always about this patient, and that is important. However, the interest of this patient is limited by the interests of other patients, since if we cannot control the virus spread, then all medical care for all patients is compromised. The medical understatement for this is triage, i.e., choosing who will and who will not be treated, a situation that has been the new standard in the Netherlands over the past year. The last stage of triage is termed code black, when even our good German neighbours have no more room for our ICU patients, and care should also be refused for people with very good chances of survival. Armand Girbes argues that less attention should be paid to COVID-19 in healthcare. The problem, however, is that COVID-19 must be prevented at an epidemic level, to avoid that covid care comprises other care.
Virus epidemiology is concerned with the virus spreading in the population. Epidemiologists are not directly concerned about the degree of illness, but mainly about how contagious someone is. After SARS-2 infections, people are most contagious from a few days before to a few days after they first become ill. This prior to onset of serious disease since the pneumonia does not appear until about a week of illness and the systemic infection with fatal outcome often even after two weeks or more.
Medical and epidemiological diagnostics are completely different worlds. The medical world sector it is about the health of the patient, the virus is less important. The best therapy in advanced disease is suppression of the immune system, for example with dexamethasone, to alleviate disease. In epidemiology, asymptomatic infected people are the major concern, because sick people stay at home or are hospitalized. Healthy infected people could spread the virus to other humans who subsequently become ill. Since January 2020 we know that asymptomatic people can spread the SARS-2 virus, similar to most other diseases, as the virus was exported from China by asymptomatic people (Figure 4).
Medical care is always about this patient, and that is important. However, the interest of this patient is limited by the interests of other patients, since if we cannot control the virus spread, then all medical care for all patients is compromised. The medical understatement for this is triage, i.e., choosing who will and who will not be treated, a situation that has been the new standard in the Netherlands over the past year. The last stage of triage is termed code black, when even our good German neighbours have no more room for our ICU patients, and care should also be refused for people with very good chances of survival. Armand Girbes argues that less attention should be paid to COVID-19 in healthcare. The problem, however, is that COVID-19 must be prevented at an epidemic level, to avoid that covid care comprises other care.
Virus epidemiology is concerned with the virus spreading in the population. Epidemiologists are not directly concerned about the degree of illness, but mainly about how contagious someone is. After SARS-2 infections, people are most contagious from a few days before to a few days after they first become ill. This prior to onset of serious disease since the pneumonia does not appear until about a week of illness and the systemic infection with fatal outcome often even after two weeks or more.
Medical and epidemiological diagnostics are completely different worlds. The medical world sector it is about the health of the patient, the virus is less important. The best therapy in advanced disease is suppression of the immune system, for example with dexamethasone, to alleviate disease. In epidemiology, asymptomatic infected people are the major concern, because sick people stay at home or are hospitalized. Healthy infected people could spread the virus to other humans who subsequently become ill. Since January 2020 we know that asymptomatic people can spread the SARS-2 virus, similar to most other diseases, as the virus was exported from China by asymptomatic people (Figure 4).

Figure 4. News item from January 26th, 2020 about SARS-2.
“The Chinese Health council said last Sunday that the virus is also contagious during the incubation period, i.e., prior to onset of disease.”. Second message tells that this fact was known by Jaap van Dissel (head of National Institute for Public Health and the Environment, Ministry of Health, Welfare and Sport – in charge of the scientific part of the national anti-SARS-2 strategy).
“The Chinese Health council said last Sunday that the virus is also contagious during the incubation period, i.e., prior to onset of disease.”. Second message tells that this fact was known by Jaap van Dissel (head of National Institute for Public Health and the Environment, Ministry of Health, Welfare and Sport – in charge of the scientific part of the national anti-SARS-2 strategy).
Infection without symptoms
Infected people can contaminate others, but most people are unaware that they are infected. The Italians already published at the beginning of the epidemic that 42.5% of infected people were asymptomatic. SARS-2 infections are difficult to detect without lab methodology. Many outbreaks come through people who were without complaints (Johansson, Tosta, Van Buul).
Scientific purists distinguish between pre-symptomatic and true asymptomatic infections: both groups have not had any complaints now and have not had any. However, the first group will become ill in the future, because their general defense is insufficient to eliminate the virus. In the second group, the virus is cleared up by the general defense. Because of their strong innate immunity, this latter group is likely to have lower virus levels.
Asymptomatic infections were already reported by China in January 2020 and implemented in the Dutch policy by Van Dissel (Figure 4). In April 2020, a warning about asymptomatic carriers appeared as a leading cause of COVID-19 spread in China. In June this was confirmed by a study from Singapore. People without complaints have on average more virus than people with COVID-19 (Figure 5). The virus peaks at about the start of the symptoms, the virus dynamics differ in innate asymptomatic people.
Isolation of symptomatic people is insufficient to stop the epidemic. From the beginning it was known that asymptomatic infections play a major role. In August 2020, it was confirmed that also young children without symptoms contribution strongly to the epidemic. Another publication confirms that message and refines the language to be presymptomatic. True asymptomatic and presymptomatic infection should be distinguished.
Scientific purists distinguish between pre-symptomatic and true asymptomatic infections: both groups have not had any complaints now and have not had any. However, the first group will become ill in the future, because their general defense is insufficient to eliminate the virus. In the second group, the virus is cleared up by the general defense. Because of their strong innate immunity, this latter group is likely to have lower virus levels.
Asymptomatic infections were already reported by China in January 2020 and implemented in the Dutch policy by Van Dissel (Figure 4). In April 2020, a warning about asymptomatic carriers appeared as a leading cause of COVID-19 spread in China. In June this was confirmed by a study from Singapore. People without complaints have on average more virus than people with COVID-19 (Figure 5). The virus peaks at about the start of the symptoms, the virus dynamics differ in innate asymptomatic people.
Isolation of symptomatic people is insufficient to stop the epidemic. From the beginning it was known that asymptomatic infections play a major role. In August 2020, it was confirmed that also young children without symptoms contribution strongly to the epidemic. Another publication confirms that message and refines the language to be presymptomatic. True asymptomatic and presymptomatic infection should be distinguished.
- Younger age strongly correlates with asymptomatic and mild infections.
- Guidelines for asymptomatic and presymptomatic infections are lacking.
- Asymptomatic cases should be reported in official COVID-19 statistics.
- Asymptomatic and presymptomatic persons carrying SARS-CoV-2 are the hidden cause of the pandemic.
Highest virus titers are found before the general immune system intervenes against the systemic infections.
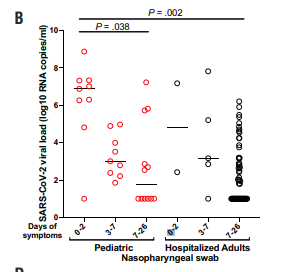
Figure 5. Virus titer in asymptomatic children and adults in the hospita
More virus
Several Western countries appear to focus at herd immunity in their epidemiological practice. The pursuit of herd immunity implies that people will be infected. The WHO has said this is unscientific and unethical. For many viral infections, herd immunity is the natural end when the maximum number of people have become ill. The strategy to get many people sick has been or is being followed in Belgium, the Netherlands, the UK, the US, and Sweden. I do not understand the potential benefit of this, as it cannot reduce the total number of infections and diseases. The Dutch strategy is to let the maximum number of people succumb to disease. It only aims at preventing a hospital overflow by too many sick people at the same time. Only a few persons from the OMT wonder whether this is a wise strategy.
Tests are primarily used on a medical indication (symptoms) and not for an epidemiological indication, i.e. contact with an infected person, although the latter is allowed possible since 1 December 2020. Disease control is based on what the care system could handle (ICU capacity), not on what is desirable, i.e., no disease. Disease prevention is not sexy in a market-driven healthcare system, because it is not directly commercial. I would like to emphasize that a commercial model would be possible, because it ultimately yields a win-win-win option for all partners.
The fight against corona makes the administrative inability of the government extra visible. These elections must be about the dismantling of the public affairs. The Netherlands has general elections on March 17, 2021. In the shortsightedness of election campaigns, prevention is the last thing politicians seem to be concerned about. Out of the 37 Dutch political parties, 0 are openly calling for zero Covid, while in Germany the largest political party aims for this. Anyone familiar with the prevention paradox knows good prevention avoids that the problem happens and will be regarded as useless (Figure 6). Providing poor prevention is better for popular votes because the coffins illustrate the need for prevention. Many people do not understand prevention, and compare lockdown measures directly with the impact of the disease, and thus fail to see proportionality. Politicians from D66 to PVV prefer to promise about nice events over prevention. Even Prime Minister Rutte illustrates that he fails to understand epidemiological prevention: "It is senseless to be tested if you have no complaints." As a result, the Netherlands remains on the course of 150 seats in the government for more virus infections and the epidemic will rage further through this country.
Tests are primarily used on a medical indication (symptoms) and not for an epidemiological indication, i.e. contact with an infected person, although the latter is allowed possible since 1 December 2020. Disease control is based on what the care system could handle (ICU capacity), not on what is desirable, i.e., no disease. Disease prevention is not sexy in a market-driven healthcare system, because it is not directly commercial. I would like to emphasize that a commercial model would be possible, because it ultimately yields a win-win-win option for all partners.
The fight against corona makes the administrative inability of the government extra visible. These elections must be about the dismantling of the public affairs. The Netherlands has general elections on March 17, 2021. In the shortsightedness of election campaigns, prevention is the last thing politicians seem to be concerned about. Out of the 37 Dutch political parties, 0 are openly calling for zero Covid, while in Germany the largest political party aims for this. Anyone familiar with the prevention paradox knows good prevention avoids that the problem happens and will be regarded as useless (Figure 6). Providing poor prevention is better for popular votes because the coffins illustrate the need for prevention. Many people do not understand prevention, and compare lockdown measures directly with the impact of the disease, and thus fail to see proportionality. Politicians from D66 to PVV prefer to promise about nice events over prevention. Even Prime Minister Rutte illustrates that he fails to understand epidemiological prevention: "It is senseless to be tested if you have no complaints." As a result, the Netherlands remains on the course of 150 seats in the government for more virus infections and the epidemic will rage further through this country.
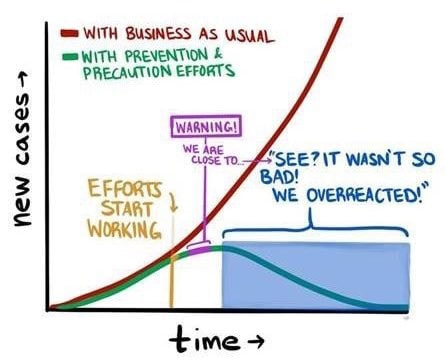
Figure 6. The prevention paradox
Less virus
The default policy against virus outbreaks is to stop the epidemic. Many European countries successfully eradicated tuberculosis. The Netherlands still has two sanatoriums and an effective test, trace and isolate (TTI) strategy. Zero tuberculosis is successfully pursued for many decades, despite the fact that tuberculosis still is endemic in other regions of this planet. The Dutch Red Team aims to stop the virus spread. Australia, New Zealand, Korea, Japan, China and many countries in South East Asia have shown that a Zero-Covid strategy can work and leads to significantly fewer casualties. Zero Covid strategies have been launched in several Western countries to stop the epidemic in 5 weeks. This encouraged people in Canada, Germany, and Ireland to call to end the epidemic. Germany had a contamination rate of 2.5 per 10,000 in the summer of 2020. The estimate is that up to 10 per 100,000 can be controlled by TTI and with extra bet also 25 / 100K. So a 4 to 10 fold overcapacity in TTI may help to control the epidemic without a lockdown, but if necessary, a lockdown can be used briefly and forcefully to regain control.
The No Covid strategy is based on liberty in green zones. The green zones are a counterpart to the red zones used in epidemics with a high death rate, such as Ebola. While the red zones are lockdown areas to occurrence of infections, the green ones opened zones that match the criteria for this. These criteria are directly linked to TTI's ability to control the epidemic. Zero is therefore a target value, but the implication of the necessity of TTI and its upscaling shows the realism of this approach to minimize the disease burden with its fatalities and morbidities.
The No Covid strategy is based on liberty in green zones. The green zones are a counterpart to the red zones used in epidemics with a high death rate, such as Ebola. While the red zones are lockdown areas to occurrence of infections, the green ones opened zones that match the criteria for this. These criteria are directly linked to TTI's ability to control the epidemic. Zero is therefore a target value, but the implication of the necessity of TTI and its upscaling shows the realism of this approach to minimize the disease burden with its fatalities and morbidities.
Endlösung.
Some people without the appropriate epidemiological knowledge consider economy and epidemic control as different choices, whereas many countries have shown that those countries that eliminate the virus have the best economic and social outcomes. These people argue that epidemic control costs a lot of money and gives great discomforts, but that only applies to ineffective measures. Ineffective measures hit hard at the economy, but the virus infections also have major economic consequences. Mortality has an economic impact through grief, but dropout due to long-term illness is directly measurable. The average duration of disease of 55 days – 8 weeks. The fear of death and disease will seriously affect consumer confidence which impact the economy. Almost everyone has contact with someone 17 to 29% of the population who is in a risk group. Many of these people will themselves take measures to prevent contamination out of respect for their loved ones.
Herstel NL[1] and the affiliated Artsen Covid Collectief[2] have raised money to campaign their strategy to establish safe zones for vulnerable people. Some concerns were raised about this plan drafted without virologists, epidemiologists, or medical scientists. I shiver at the thought that vulnerable people would then be locked up in a kind of concentration camp where they ought to be safe without an end date of the ongoing epidemic (see Virus epidemiology above). Ought to be because people from the unsafe outside world keep dropping in as caregivers or as loved relatives. Thus the ‘wall of protection’ may resemble a burial coffin. Sylvain Ephimenco and Talitha Muusse openly suggest that we can let people die to try to save the economy. The disdain for ethics after the Nuremberg trials is dispicted in Endlösung: sacrificing fellow human beings for your own gain. When we said "Niemals wieder", we also referred to this aspect of Nazism and evolutionary humanism. When my rage calms, I realize that this solution is not only unethical, but also impractical:
[1] A broad collective of physicians, economists, entrepreneurs, policy scientists, psychiatrist. This platform does not contain any medical scientist like virologist or epidemiologist.
[2] A group of some physicians
Herstel NL[1] and the affiliated Artsen Covid Collectief[2] have raised money to campaign their strategy to establish safe zones for vulnerable people. Some concerns were raised about this plan drafted without virologists, epidemiologists, or medical scientists. I shiver at the thought that vulnerable people would then be locked up in a kind of concentration camp where they ought to be safe without an end date of the ongoing epidemic (see Virus epidemiology above). Ought to be because people from the unsafe outside world keep dropping in as caregivers or as loved relatives. Thus the ‘wall of protection’ may resemble a burial coffin. Sylvain Ephimenco and Talitha Muusse openly suggest that we can let people die to try to save the economy. The disdain for ethics after the Nuremberg trials is dispicted in Endlösung: sacrificing fellow human beings for your own gain. When we said "Niemals wieder", we also referred to this aspect of Nazism and evolutionary humanism. When my rage calms, I realize that this solution is not only unethical, but also impractical:
- It will be hard to isolate vulnerable people from carers, their loved ones, and the rest of society.
- Manaus has shown that society is not going to get herd immunity because infection does not produce sterilizing immunity.
- A fair proportion of less vulnerable people get sick from COVID if the vulnerable are protected, like in Israel after the vaccination of the over-60s.
- It is a major challenge to create a safe place for more than 4 million vulnerable fellow countrymen. Certainly, if one considers that quarantine vulnerable people failed to work in the first wave.
- The economic consequences of such a policy are disastrous. Countries that do have some ethical standards will close the borders to a country that follows such a strategy. Europe has repeatedly shown on less loaded topics, such as veterinary virus epidemics, that an uncontrolled situation in addition to a controlled situation leads to isolation of the area - which is economically disastrous.
- The costs of this solution are unprecedented, if 625,000 healthy people with co-morbidities would be on sick leave for an undetermined period.
[1] A broad collective of physicians, economists, entrepreneurs, policy scientists, psychiatrist. This platform does not contain any medical scientist like virologist or epidemiologist.
[2] A group of some physicians
Desperate disease
The saying “desperate diseases call for desperate measures” reunites medical and epidemiological science. Poor prevention allows virus spread through the population (Figure 6). A failing lockdown is the worst-case scenario, especially if the lockdown extended for years. Poor prevention implies more lockdown measures and more victims causing economic damage.
The common cold epidemics in temperate regions teach us that coronaviruses cause many infections in winter and few in summer. The virus remains stable at low temperatures in dry air with little sunlight. The respiratory tract is vulnerable to low temperatures, dry air, vitamin D deficiency and air pollution, mostly wood smoke. Many factors contribute to contain the virus in the summer and allow the epidemic to thrive in the winter.
If the virus is not eradicated, countries must keep fighting the virus. As a result, the lockdown will last a year or several years, possibly less in the summer because coronaviruses - we know them from colds - then spread less well. The result is that risk groups have been indoors alone for months because they have no choice. Most elderly stay in quarantine and sometimes they die alone. That has only gotten worse.
As soon as the number of new infections decreases, many governments, like the Dutch opt for releasing measures. The economic damage is mainly caused by the yo-yo effect and the lack of consumer confidence. A better strategy is to continue with the measures to fully control the virus with test, trace and isolate (TTI). This requires a low number of infections in society, but gives people back the freedom because it has minimal impact on society and maximum effectiveness.
The common cold epidemics in temperate regions teach us that coronaviruses cause many infections in winter and few in summer. The virus remains stable at low temperatures in dry air with little sunlight. The respiratory tract is vulnerable to low temperatures, dry air, vitamin D deficiency and air pollution, mostly wood smoke. Many factors contribute to contain the virus in the summer and allow the epidemic to thrive in the winter.
If the virus is not eradicated, countries must keep fighting the virus. As a result, the lockdown will last a year or several years, possibly less in the summer because coronaviruses - we know them from colds - then spread less well. The result is that risk groups have been indoors alone for months because they have no choice. Most elderly stay in quarantine and sometimes they die alone. That has only gotten worse.
As soon as the number of new infections decreases, many governments, like the Dutch opt for releasing measures. The economic damage is mainly caused by the yo-yo effect and the lack of consumer confidence. A better strategy is to continue with the measures to fully control the virus with test, trace and isolate (TTI). This requires a low number of infections in society, but gives people back the freedom because it has minimal impact on society and maximum effectiveness.
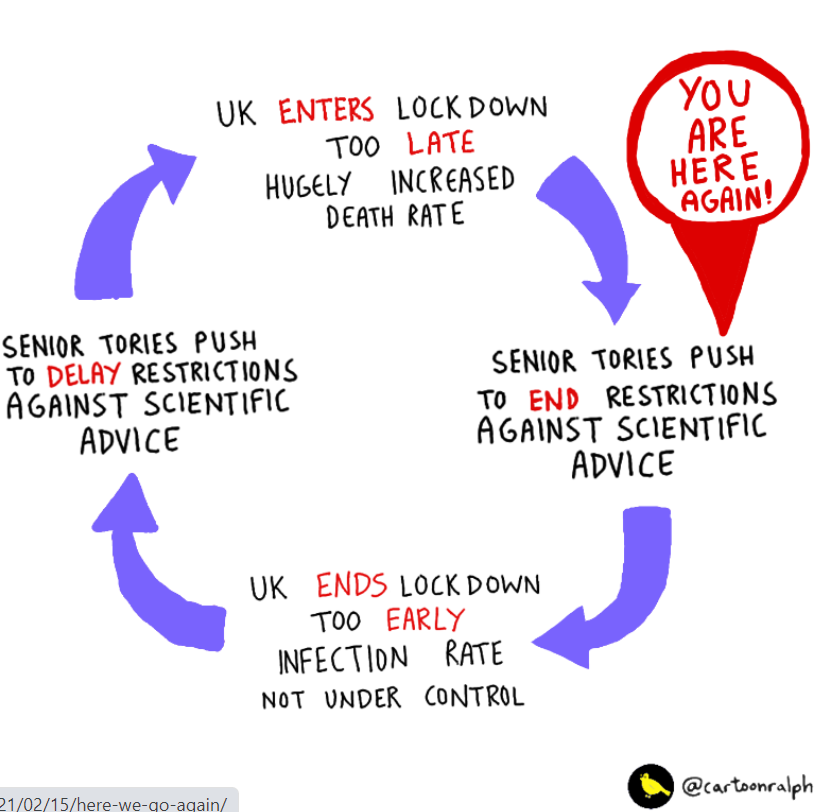
Figure 7. Cycle of not maintaining the “desperate diseases call for desperate measures” mantra allowing the epidemic to continue
Targeted approach
SARS-2 is difficult to control because many infections occur by people without symptoms (asymptomatic). Some develop symptoms later (presymptomatic), others never (real asymptomatic infections). Therefore, test, trace and isolate (TTI) is crucial. This also applies to asymptomatic infections in children. During the epidemic, the number of asymptomatic and presymptomatic infections increases, causing the virus to spread even more unnoticed. Although testing based on contact research (TTI) has been permitted since 1st of December 2020 in the Netherlands, it is not yet the standard. It is worrying that the Netherlands is not yet fully committed to TTI, despite previous advice such as in Lesson Learned in August 2020.
Fighting a disease is easier when less people are infected, the more people are infected, the more difficult it is to protect vulnerable people. Vaccination prevents disease in 60 to 95% of people, depending on the vaccine. Maybe the numbers may be slightly lower in practice, as is seen for most drug research. However, vaccinated people are neither fully protected against disease, nor (long-term) protected against infection. It remains necessary to combat the epidemic. The concept of the idea to require negative test result for all travelers from high-risk areas is still valid.
An effective method is to use rapid tests in places where people meet, possibly in combination with other tests. Appropriate selection would be staff from hospitals, nursing homes and schools. Not everyone needs monitoring staff with rapid tests will give a clear indication of what is going on. Positive tests could invoke isolation, ask for confirmation and test all contacts (Figure 7). A gargle test can help make to make sampling less invasive for people. A Zero Covid strategy will allow larger gatherings of healthy people in the green zones – think of such as sport events, visits to music concerts, church meetings, theme park visits, shopping streets, air travel and so on. Anyone can be tested on the spot, if the Zero Covid has not yet been broken.
Aim for Zero Covid is logical, effective and the default strategy in virus epidemiology. Lockdown measures can be effective but have many side effects for the economy and society. Staff of German care homes undergo daily rapid tests. This could be extended to schools and other places where many people meet. Queueing for days to be tested undermines the concept of testing for TTI. Merkel shows her vision to open up Germany: reduce the epidemic to the level that TTI can detect every day. This requires a TTI overcapacity because the freedom of society depends on it. Merkel illustrates by her calculation that she understands exponential calculation – a deficit in many other leaders. She understands that scaling up TTI capacity is the best support for economy and society.
Fighting a disease is easier when less people are infected, the more people are infected, the more difficult it is to protect vulnerable people. Vaccination prevents disease in 60 to 95% of people, depending on the vaccine. Maybe the numbers may be slightly lower in practice, as is seen for most drug research. However, vaccinated people are neither fully protected against disease, nor (long-term) protected against infection. It remains necessary to combat the epidemic. The concept of the idea to require negative test result for all travelers from high-risk areas is still valid.
An effective method is to use rapid tests in places where people meet, possibly in combination with other tests. Appropriate selection would be staff from hospitals, nursing homes and schools. Not everyone needs monitoring staff with rapid tests will give a clear indication of what is going on. Positive tests could invoke isolation, ask for confirmation and test all contacts (Figure 7). A gargle test can help make to make sampling less invasive for people. A Zero Covid strategy will allow larger gatherings of healthy people in the green zones – think of such as sport events, visits to music concerts, church meetings, theme park visits, shopping streets, air travel and so on. Anyone can be tested on the spot, if the Zero Covid has not yet been broken.
Aim for Zero Covid is logical, effective and the default strategy in virus epidemiology. Lockdown measures can be effective but have many side effects for the economy and society. Staff of German care homes undergo daily rapid tests. This could be extended to schools and other places where many people meet. Queueing for days to be tested undermines the concept of testing for TTI. Merkel shows her vision to open up Germany: reduce the epidemic to the level that TTI can detect every day. This requires a TTI overcapacity because the freedom of society depends on it. Merkel illustrates by her calculation that she understands exponential calculation – a deficit in many other leaders. She understands that scaling up TTI capacity is the best support for economy and society.
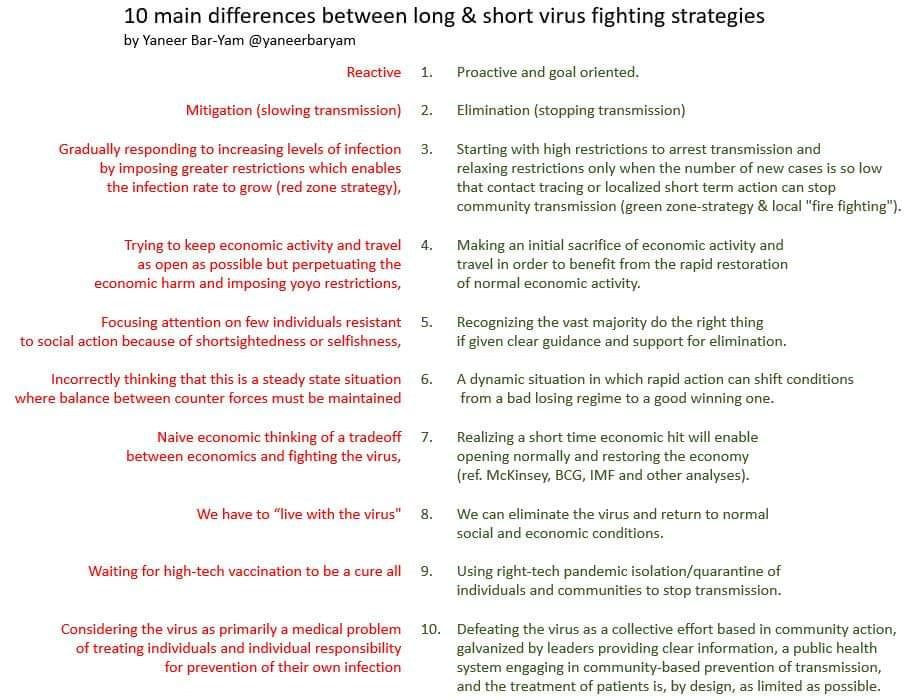
Figure 8. Differences between a fast effective and a slow ineffective strategy against the epidemic..
Schools
The wrong strategy of herd immunity hijacked the schools open discussion. Some virologists suggested that children are important for building herd immunity. They understand that children spread the disease. This directly contradicts the concept of safe education. Children without symptoms have higher virus titers than adults in the hospital (Figure 4). COVID-19 is not harmless in children, so it is unwise to have many children infected.
The Netherlands has a fierce discussion about schools open or closed with many improper and incorrect arguments. I am in favour of opening schools safely and not first open schools and later see it if could be done safely in pilots. This implies daily testing of the staff and keeping distances between the students. In the limited space available in schools, this could ask for solutions like limiting the time at school to halve or a quarter of normal time. For children’s (social) health there is no need to have full-time lessons in a class with 30 pupils. Most educational backlog could also be prevented with a hybrid education combining teaching within the room with video and online classes.
The Netherlands has a fierce discussion about schools open or closed with many improper and incorrect arguments. I am in favour of opening schools safely and not first open schools and later see it if could be done safely in pilots. This implies daily testing of the staff and keeping distances between the students. In the limited space available in schools, this could ask for solutions like limiting the time at school to halve or a quarter of normal time. For children’s (social) health there is no need to have full-time lessons in a class with 30 pupils. Most educational backlog could also be prevented with a hybrid education combining teaching within the room with video and online classes.
Mutants
A high virus circulation causes many virus mutants to evolve. In an unprotected population, new variants will evolve that spread faster. In a partially protected population, e.g., by infection or vaccination, mutants that evade the immune system will be selected, similar to the evolution of bacteria under a moderate dose of penicillin towards antibiotic resistance. In summary, the selection at SARS-2 focuses on:
The virological certainty that mutants will emerge and that evolutionary pressures are more likely to lead to more virulent variants and reinfections shows that halting the epidemic is the only sustainable solution. Nobody wants a SARS-2.1 or SARS-3.0 epidemic. The evolutionary tricks of coronaviruses surpass those of the Spanish flu, that had multiple epidemics, causing more deaths in some later ones.
- Viruses that spread faster due to stronger binding to the receptor.
- Viruses that later delay symptoms by evading the innate immune systems, such as interferon.
- Viruses that evade specific defenses such as antibodies and virus-specific T cells.
- British variant B.1.1.7 is more contagious and evades the specific and innate immune system causing more hospital admissions.
- South African variant B.1.351 (501Y.V2) is more contagious and evades the specific immune system.
- Californian variant B.1.429 is increasingly common, but it is unclear why.
- Brazilian variant B.1.1.248 evades defense.
The virological certainty that mutants will emerge and that evolutionary pressures are more likely to lead to more virulent variants and reinfections shows that halting the epidemic is the only sustainable solution. Nobody wants a SARS-2.1 or SARS-3.0 epidemic. The evolutionary tricks of coronaviruses surpass those of the Spanish flu, that had multiple epidemics, causing more deaths in some later ones.
Virus Ethics
Effective and open
Do we strife for the good things?
Beyond mortality
Special immunity
Vaccination
Prevention of epidemic
Effective and open
Do we strife for the good things?
Beyond mortality
Special immunity
Vaccination
Prevention of epidemic
